
AVSL MULTI BROWN SNAKE ANTIVENOM
• Fast working antivenom which produces best results with prompt treatment
• Australia’s manufacturer of veterinary specific AVSL Multi Brown Snake Antivenom
• Processed in our own APVMA accredited laboratory
• Available in 5mL /800 units and 10mL /1600 units
CLINICAL SIGNS OF BROWN SNAKE ENVENOMATION
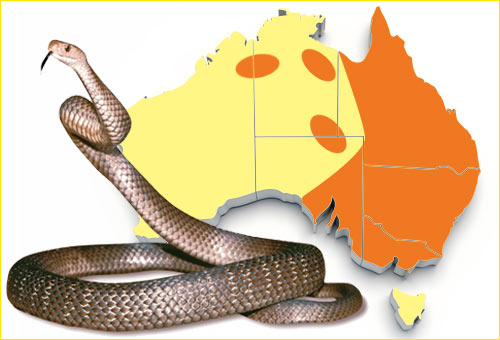
There are several venomous Brown Snakes (Pseudonaja spp.) found throughout Australia all of which can be fatal to both domestic and production animals.
The common or Eastern Brown Snake Pseudonaja textilis is widespread throughout Eastern Australia being found in most of Queensland, New South Wales and Victoria. It is also found in South Australia and pockets of the Northern Territory. See the AVSL Snake Identification Chart.
SNAKE IDENTIFICATION
There are several venomous Brown Snakes (Pseudonaja spp.) found throughout Australia all of which can be fatal to both domestic and production animals.
The common or Eastern Brown Snake Pseudonaja textilis is widespread throughout Eastern Australia being found in most of Queensland, New South Wales and Victoria. It is also found in South Australia and pockets of the Northern Territory. See the AVSL Snake Identification Chart.
Western Brown Snakes (nuchalis – complex) are found throughout Western Australia, South Australia and western New South Wales. Three species of western brown snakes exist, Pseudonaja mengdeni, Pseudonaja aspidorhyncha and Pseudonaja nuchalis.
The Dugite Pseudonaja affinis is found in the far southwest corner of Western Australia and extending into South Australia.
Brown Snake venom is typical of elapid venoms being comprised of different toxins including low molecular weight substances, various enzymes, coagulants, neurotoxins (presynaptic and postsynaptic), haemolysins and myolysins and cytotoxins. Neurotoxins and coagulants are the most important components.
Envenomated animals become paralysed and death usually ensues due to ventilatory failure and or as a result of a venom-induced consumptive coagulopathy.
Some species are more susceptible to Brown Snake venom than others eg dogs more susceptible than cats.
Identify the snake if presented using the AVSL Snake Identification Chart. Western Brown Snake (nuchalis complex) identification (Western Brown Snakes)
Alternatively use a snake venom detection kit swabbing the bite site (rarely found) or urine or blood.
CLINICAL SIGNS OF BROWN SNAKE ENVENOMATION
The rate of progression is highly variable and depends on several factors including patient body size, physiological status, snake venom potency and the dose of venom delivered.
Differential Diagnosis
Includes all causes of lower motor neurone paralysis – tick paralysis, tetrodotoxins, ciguiatera, polyrediculoneuritis, organophosphate or carbonate intoxication, thromboembolic disease and meningitis/myelitis.
CLINICAL SIGNS IN DOGS
- Pre-paralytic signs due to rapid diffusion of low molecular weight toxins – vomiting, initial collapse, salivation mydriasis, trembling within a few minutes followed by an apparent ‘recovery’. Indicates a potentially lethal envenomation.
- Serious consumptive coagulopathy due to procoagulants in venom – bleeding from bite site and or venipuncture sites, gingival pettechiae, hyphaema, prolonged activated clotting times, low fibrinogen and platelet numbers.
- Other signs can be diverse and include mydriasis with slower pupillary light responses, vomiting, haematomesis, severe trembling, salivation, excitement, salivation, defecation, posterior paresis leading to a generalised flaccid paralysis, cyanosis and death.
CLINICAL SIGNS IN CATS
- Can be varied and inconsistent.
- Preparalytic collapse infrequently seen in cats. Usually the earliest signs are weakness and ataxia. Other signs include hind limb paralysis, ataxia, vomiting, absent pupillary light reflex, mydriasis, tachypnoea, depression, coma and bleeding from the bite site.
- Most often cats are presented with a generalised flaccid paralysis but retain the ability to move their tail.

TREATMENT
All envenomated patients should have an intravenous catheter placed and Hartmanns or normal saline administered. Correct any dehydration then continue at 1 – 1.5 times maintenance to maintain normovolaemia and consequently blood pressure and cardiac output and maintain glomerular filtration rate and assist in offsetting possible renal toxicity due to myoglobinaemia. See the AVSL Fluid Chart.
TREATMENT
- Administration of an appropriate dose of brown snake antivenom as soon as possible. 1600units AVSL Multi Brown Snake Antivenom will neutralise the average yield of an adult brown snake. Cases that have experienced a pre paralytic collapse and advanced cases may require more than one vial initially. Dilute antivenom 1-2 x in Saline or Hartmanns and administer intravenously slowly over at least 20 minutes.
- If possible collect a pre treatment blood sample to assess packed cell volume, total protein, serum colour, activated clotting time.
- Activated Clotting time can be performed at initial presentation and if prolonged and antivenom is administered it should be re-evaluated 6hrs later. Further vials of antivenom should be given if still prolonged.
- Use SpO2 to determine if supplementary oxygen therapy may be necessary, ventilation may be necessary in advanced cases
USEFUL LINKS
Good description of different types of snake envenomation in domestic animals